
Knee Arthroscopy
ACL (Anterior Cruciate Ligament) Repair
Introduction
Anatomy
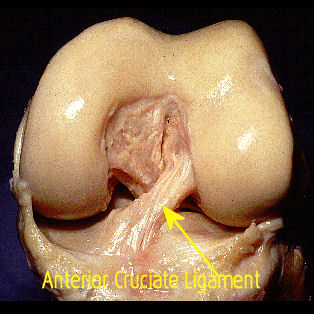
Cruciate ligaments (also cruciform ligaments) are pairs of ligaments arranged like a cross in the knee joint. Cruciate ligaments of the knee are the Anterior cruciate ligament(ACL) and the Posterior cruciate ligament (PCL). These ligaments are two strong, rounded bands that extend from the head of the tibia to the intercondyloid notch of the femur. The ACL is lateral and the PCL is medial. They cross each other like the limbs of an X. The ACL and PCL remain distinct throughout and each has its own partial synovial sheath.
Injury to the anterior cruciate ligament (ACL) can be devastating. It generally occurs in younger patients, and misdiagnosis, delayed diagnosis, recurrent injury, and improper surgical technique may leave a teenage athlete with a knee that is destined to develop premature arthritis. Fortunately, perspectives on the management of ACL-injured knees are changing.
Function
Relative to the femur, the ACL keeps the tibia from slipping forward and the PCL keeps the tibia from slipping backward.The ACL originates from the medial and anterior aspect of the tibial plateau and runs superiorly, laterally, and posteriorly toward its insertion on the lateral femoral condyleThe ACL consists of individual fiber bundles, named for their insertion points on the tibial footprint. The larger anteromedial (AM) bundle inserts anteromedially on the tibial side and originates more proximally on the femoral side than the posterolateral (PL) bundle, which is posterolateral relative to AM bundle.
Studies indicate that the AM bundle tightens in flexion while the PL bundle relaxes; in extension, the PL bundle tightens while the AM bundle relaxes… In extension, their insertion points are vertical to each other, but with the knee in 90 degrees flexion, the insertion points are horizontal to each other. Likewise, the bundles themselves shift from parallel orientation in extension to crossed orientation in flexion.
Mechanism of Injury
ACL injuries can have contact or, more frequently, noncontact mechanisms of injury. They may occur with internal or external rotation maneuvers. Noncontact injuries generally involve a deceleration, change-of-direction maneuver. Patients usually recollect a sensation of the knee buckling and collapsing to the ground.An audible pop or tearing sensation is heard in 80% of acute ACL injuries.
The knee frequently develops a hemarthrosis within 3 hours, but in some patients there may be a gradual onset of swelling over 24 hours. In an acutely injured knee, meniscal tears occur more frequently laterally than medially) In the chronic setting, medial meniscal tears occur more frequently.
Treatment
Traditionally treatment of ACL tear involve new reconstruction th tendon grafts from hamstrings, patellar tendon etc. Single-Bundle ACL reconstruction, a graft is used to basically replicate the positioning of the AM bundle. The Double-Bundle technique uses two separate grafts to replicate the positioning of both the AM and the PL bundles. Because the AM bundle makes a greater contribution to anteroposterior knee stability, while the PL bundle makes a greater contribution to rotational stability, a double-bundle technique may be better able to restore normal knee kinematics.
Meniscus - Menisectomy / Meniscus Repair
Meniscus (cartilage) Surgery
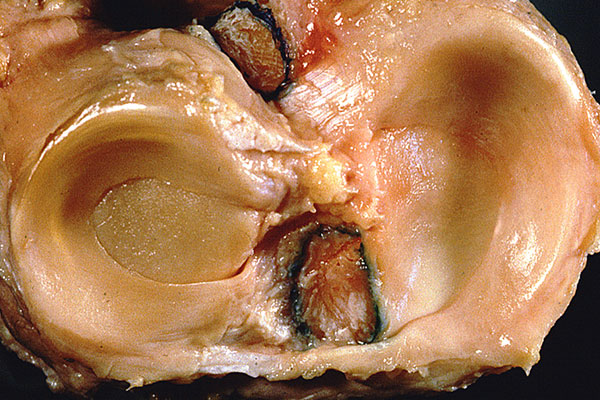
The knee has two crescent shaped shock absorbing cartilages, the menisci. The thin, tapered edge is susceptible to tears. The torn part can move in and out of the weight-bearing area and cause locking and/or catching of the joint, and pain. Most often, these tears do not heal spontaneously.
Treatment focuses on preservation of as much functional cartilage as possible, to maintain the shock absorbing function.
The torn, unstable, nonfunctional piece of cartilage is usually removed (Menisectomy) through a 2 – 3mm incision, using a variety of arthroscopic instruments. On occasion, the torn part is repairable (Meniscus repair). Particularly in young and/or athletic individuals. The initial rehabilitation is slower than after removal of the torn part. It is anticipated that repair will lead to better results in the long run.
Meniscus surgery typically takes 30-45 minutes. After excision of the torn part, rehabilitation can be swift, only limited by discomfort. Most people use crutches for the first few days, walk fairly well by the end of the first week, and are ready to consider some exercise by two weeks. The knee remains somewhat painful with activity for several months. A “reminder” that surgery was performed!
After isolated meniscal repair, most often I ask to limit bending of the knee to 45 degrees for six weeks, to protect the repair. Weight-bearing can be initiated immediately.
Posterior Cruciate Ligament
Meniscus (cartilage) Surgery
The posterior cruciate ligament (or PCL) is one of the four major ligaments of the knee. It connects the posterior intercondylar area of the tibia to the medial condyle of the femur. This configuration allows the PCL to resist forces pushing the tibia posteriorly relative to the femur.The PCL is an intracapsular ligament along with the anterior cruciate ligament (ACL) because it lies deep within the knee joint. They are both isolated from the fluid-filled synovial cavity, with the synovial membrane wrapped around them. Along with the ACL which keeps the tibia from sliding too far forward, the PCL helps to maintain the tibia in position below the femur .bone. Posterior cruciate ligament injuries comprise between 3% and 20% of all knee ligament injuries.
Common causes include
Striking the knee against the dashboard during an auto accidentThis occurs when the knee is bent, and an object forcefully strikes the shin backwards. It is called a ‘dashboard injury’ because this can be seen in car collisions when the shin forcefully strikes the dashboard.
Falling on the knee while it’s bent. The other common mechanism of injury is a sports injury when an athlete falls on the front of their knee. In this injury, the knee is hyperflexed (bent all the way back), with the foot held pointing downwards. These types of injuries stress the PCL, and if the force is high enough, a PCL tear will result. These injuries are especially common in football, soccer, baseball, skiing etc.
Classification of PCL injuries
- Grade I : The PCL has a partial tear
- Grade II : The ligament is partially torn and is looser than in Grade I
- Grade III : The ligament is completely torn and the knee becomes unstable
- Grade IV : The PCL is damaged along with another ligament in the knee
Shoulder Arthroscopy
Anatomy

Shoulder is a complex joint that is capable of more motion than any other joint in your body. It is made up of three bones: upper arm bone (humerus), shoulder blade (scapula), and collarbone (clavicle).
Ball and Socket
The head of humerus bone fits into a rounded socket-glenoid in shoulder blade.. A slippery tissue called articular cartilage covers the surface of the ball and the socket. It creates a smooth, frictionless surface that helps the bones glide easily across each other.The glenoid is ringed by strong fibrous cartilage called the labrum. The labrum forms a gasket around the socket, adds stability, and cushions the joint.
Shoulder capsule
The joint is surrounded by bands of tissue called ligaments. They form a capsule that holds the joint together. The undersurface of the capsule is lined by a thin membrane called the synovium. It produces synovial fluid that lubricates the shoulder joint.
Rotator cuff
Four tendons surround the shoulder capsule and help keep arm bone centered in shoulder socket and they help move shoulder in different directions. The tendons in the rotator cuff can tear when they are overused or injured. The cuff covers the head of the humerus and attaches it to shoulder blade.
Bursa
There is a lubricating sac called a bursa between the rotator cuff and the bone on top of shoulder (acromion). The bursa helps the rotator cuff tendons glide smoothly when one move his arm.
Various conditions which require shoulder arthroscopy
Rotator Cuff Tear
This can be treated with either arthroscopy or open procedure. Which method is better, is controversial, it depends on the severity of tear and surgeons experience and comfort.
The edges of the muscles are brought together. The tendon is attached to the bone with sutures. Small suture anchors are often used to help attach the tendon to the bone. The anchors can be made of titanium or bioabsorable material .They do not need to be removed after surgery.
Shoulder Instability
Labral tears, such as Bankart tear & SLAP taer, are commonly treated with arthroscopy. The Bankart lesion is a tear on the labrum in the lower part of the shoulder joint. A SLAP lesion involves the labrum and the ligament on the top part of the shoulder joint.
It is very important that patients who have arthroscopic surgery for these procedures follow their post-operative rehab protocol very closely.
Impingement Syndrome
Patients with shoulder bursitis, also called impingement syndrome, that is not cured with simple treatments may consider a procedure called an arthroscopic subacromial decompression. This procedure removes the inflamed bursa and some bone from the irritated area around the rotator cuff tendons. By removing this tissue, more space is created for the tendons and the inflammation often subsides.
Biceps Tendonitis
The biceps tendon can become irritated and inflamed as an isolated problem or in association with problems such as impingement syndrome and rotator cuff tears. When the biceps tendon is damaged and causing pain, a procedure called a tenodesis can be performed. This procedure usually causes no functional difference, but often relieves symptoms.
Frozen Shoulder
Frozen shoulder seldom requires operative treatment, and treatment for many months or years is often necessary before considering operative treatment. When frozen shoulder must be treated surgically, it is of utmost importance to begin aggressive physical therapy immediately following surgery. Without this, it is likely the problem will return.
Acromio-Clavicular Joint Arthritis
Arthroscopy of the hip uses specialized arthroscopic instruments to treat various unusual disorders of the hip. The primary indications for hip arthroscopy
- Removal of loose bodies (usually cartilage)
- Debridement/repair of labral tears (the labrum is an O-ring of cartilage around the hip socket)
- Removal of bone spurs that cause hip pain (femoral or acetabular spurs)
- Removal of pathologic synovium (joint lining)
- Sometimes hip arthroscopy can provide a diagnosis when other means (e.g., MRI) fail
- Hip arthroscopy with thermal shrinkage has proved useful in persons with instability of the hip
- Femoroacetabular impingement, which is the removal of painful bone spurs around the hip
- People who have pain that can be localized to the hip, but with minimal findings on x-ray
Procedure Details
The patient, after being anesthetized, is placed in traction on a specialized operating room table. The traction is necessary to pull the hip apart slightly to allow us to insert instruments into the joint safely, without injuring the cartilage. All this is done with the help of a portable x-ray machine to make sure the instruments are positioned correctly. A pump device is used to fill the joint with saline. Then an arthroscope is used to view the joint; once a problem is identified, it is treated with a variety of instruments. It includes :- Treatment of the Labrum: Labral tears are treated during hip arthroscopy with either refixation (repair of the labral tissue using suture) or debridement (removal of a small portion of the labrum), depending on the tear type and the patient’s age.
- Shaving of the Bone: When abnormalities of the bony shape of the hip ball or socket occur, such as in FAI or hip impingement. specialized bone shavers are used to remove the excess bone and recontour the hip.
- Removal of Inflamed Tissue: Most of the pain you feel from you hip is due to nerve endings that have become irritated in the presence of inflammation. Much of this inflamed tissue is torn labrum and synovium, the lining of the joint. This inflamed tissue is shaved away during hip arthroscopy.
Ankle arthroscopy is a surgical procedure that uses a fiber-optic viewing camera and small surgical tools to operate in and around the ankle joint through small incisions. Ankle arthroscopy is performed for the surgical evaluation and treatment of a variety of ankle conditions. Arthroscopic surgery can have a quicker recovery time than traditional open surgery.
Indicated in- Osteochondral lesions of the talus
- Microfracture of OCD
- Debridement of post-traumatic synovitis
- ATFL anterolateral impingement
- AITFL( antero-inferior tibiofibular ligament) anterolateral impingement
- Resection of anterior tibiotalar spurs– anterior bony impingement
- OS trigonum excision
- Removal of loose bodies
- OS trigonum excision
- Arthrofibrosis
- OS trigonum excision
- Unexplained Ankle Symptoms
- Cartilage debridement in conjunction with ankle fusions
Procedure
Ankle arthroscopy is generally performed as an day care surgery under general anesthesia with or without a regional pain block or epidural anesthesia with sedation. After adequate anesthesia is established, a tourniquet is applied to the leg and the leg is prepped and draped in a sterile fashion. Mechanical distraction devices are sometimes used to help surgeons temporarily enlarge the potential space of the ankle. After the foot and ankle are appropriately positioned, at least two, approximately 0.5mm incisions are made in the ankle. These incisions become the entry sites into the ankle, or portals, for the arthroscopic camera and instruments. These portals are placed strategically in an effort to avoid vessels and nerves. The incisions are made in the front or back of the ankle, or a combination of these. Sterile fluid is then allowed to flow through the ankle to further open the joint. The camera and instruments can then be exchanged between portals to perform the surgery. At the conclusion of the procedure, small sutures are placed in the skin to close the portals.